You've probably had this moment already. You do a question block, read a vignette, correctly identify the diagnosis, and still miss the item. Then you review the explanation and realize the test wasn't really asking, “What disease is this?” It was asking, “What disease is this, what osteopathic finding matters, and which answer is most defensible in the way NBOME likes to think?”
That's why COMLEX Step 1 questions feel so frustrating at first. They don't just test knowledge. They test whether you can sort through a mixed clinical vignette, notice the osteopathic layer, and avoid answer choices that look reasonable but aren't the one best answer.
I've watched a lot of students hit the same wall. They've done plenty of UWorld, they know the pathology, and they still feel thrown off by COMLEX wording, OMM integration, ethics framing, or the way distractors are written. The good news is that this style is learnable. Once you see the logic behind COMLEX Step 1 questions, the exam stops feeling random.
Why COMLEX Questions Feel So Different
A common scenario looks like this.
You get a stem about a patient with chest pain after vomiting. You think Boerhaave syndrome. Good diagnosis. Then the answer choices include autonomic findings, viscerosomatic levels, lymphatic considerations, and a management choice that would be correct in a more USMLE-style question. You pick the disease-based answer and miss the item because COMLEX wanted you to identify the osteopathic implication inside the same vignette.
That's the part that unsettles people. The question feels like it changed genres halfway through.
The hidden second question
A lot of COMLEX Step 1 questions contain two layers:
- The core medical problem
- The osteopathic or exam-specific overlay
If you only answer the first layer, you'll often narrow to two choices and still pick the wrong one. That's why students say COMLEX feels “vague.” It usually isn't vague. It's just asking for a broader frame than the one many Qbanks train you to use.
For students deciding how much their USMLE prep overlaps, this matters. A side-by-side comparison of COMLEX and USMLE for DO students is useful, but the lived experience is even simpler: COMLEX expects you to think like a clinician who also notices osteopathic structure, autonomics, and patient context in the same pass through the stem.
COMLEX often punishes partial understanding that would still earn you points on another exam.
Why that's not a flaw
It helps to stop treating this as bad question writing. COMLEX is built to test a distinct clinical mindset. The exam wants to know whether you can move between foundational science, patient presentation, and osteopathic reasoning without acting as if they live in separate folders.
That's also why students can feel strong on content but shaky on performance. You may know the micro, pharm, pathology, and physiology. What you haven't practiced enough is the switch in question logic.
Once you start reading COMLEX items with this question in mind, things get clearer: What is the standard medical answer, and what extra osteopathic clue changes the best choice? That single habit fixes a surprising number of misses.
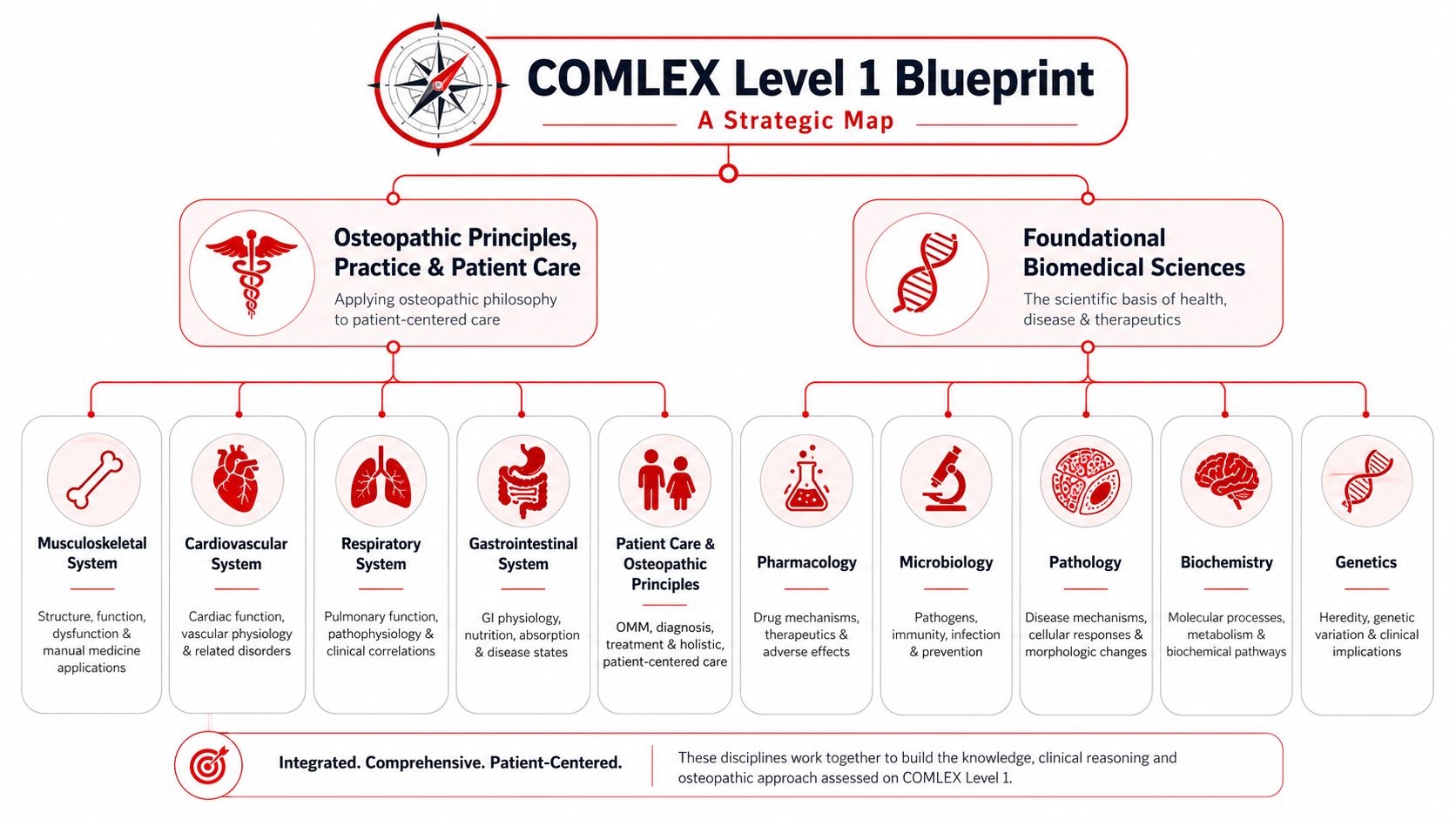
Deconstructing the COMLEX Level 1 Blueprint
Before you get better at COMLEX Step 1 questions, you need a clean mental model of the exam you're taking. A lot of stress comes from studying for an abstract “boards” concept instead of a specific testing structure.
What the day looks like
The exam has historically been 352 multiple-choice questions split into 8 sections of 44, delivered in a one-day, nine-hour testing experience with two 4-hour sessions, a 16-minute pre-exam tutorial, and 60 minutes of pooled break time across three scheduled breaks according to this COMLEX Level 1 format guide.
That same guide notes a future structural change. Starting May 7, 2026, NBOME will reduce the exam to 320 questions arranged as 8 sections of 40 while keeping the eight-hour testing window. The same source describes this as a major pacing change that will alter how students manage sections on test day.
If you're testing before that date, study for the current format assigned to your administration. If you're testing after that date, prepare for the revised one.
The blueprint is a map, not a list
Students often ask, “What subjects are on COMLEX?” That's the wrong first question. A better one is, “How does COMLEX combine subjects?”
Think of the blueprint as two overlapping dimensions:
| Dimension | What it means for questions |
|---|---|
| Foundational biomedical sciences | Anatomy, physiology, pathology, pharmacology, microbiology, and related basic science concepts appear through clinical application |
| Osteopathic principles and patient care | OMM, structural findings, autonomics, and osteopathic reasoning can appear as the main topic or as an embedded clue |
That's why a question can feel like pathology at first and then turn into an OMM item by the last sentence.
For a broader study framework, many students benefit from a dedicated COMLEX Level 1 study guide for DO students, especially when they need to align content review with question style rather than treating those as separate tasks.
What this means for pacing
The blueprint matters because pacing is never just about speed. It's about switching modes efficiently.
On COMLEX, you might move from a standard physiology item to a musculoskeletal question with structural findings, then to an ethics vignette, then to an audiovisual item. That variety creates fatigue long before pure content does.
A practical approach is to train in mixed blocks and ask yourself after every miss:
- Was this a knowledge gap
- Was this a question-type recognition problem
- Did I ignore the osteopathic layer
- Did I rush and choose the first defensible answer rather than the best one
Practical rule: Your study plan should mirror the exam's mixed logic, not just its subject list.
COMLEX vs USMLE Questions Key Differences
Students who prepare for both exams often assume high USMLE-style performance will automatically carry over. It helps, but it doesn't fully transfer.
There is a relationship between the exams. Research cited in a discussion of COMLEX performance reports a correlation coefficient of about 0.75 between COMLEX and USMLE scores, and students who took the exams within 1 to 7 days of each other had a median COMLEX score of 646 versus 491 for those who waited longer according to this discussion summarizing the data. Even with that overlap, the same source highlights that distinct preparation strategy still matters.
How the questions feel different
Here's the practical comparison students notice during question review:
| Feature | COMLEX tendency | USMLE tendency |
|---|---|---|
| OMM content | Directly tested and often integrated into non-OMM cases | Not a focus |
| Answer logic | Often asks for the most osteopathically complete answer | Often rewards tighter disease-based reasoning |
| Distractors | Frequently include plausible “almost right” choices from another frame | Often cleaner separation between right and wrong |
| Clinical framing | May shift from standard diagnosis to structure-function implications | More consistently centered on core diagnosis and management logic |
| Buzzwords | Can mislead if you stop at pattern recognition | More often helpful when paired with pathophysiology |
Buzzwords are less trustworthy on COMLEX
A lot of students get burned here.
On a USMLE-style question, a classic clue may push you quickly toward the diagnosis and that may be enough. On COMLEX, the writers may give you the clue, let you identify the disease, and then ask about a viscerosomatic level, a rib dysfunction pattern, a counterstrain setup, or the most osteopathically compatible next conclusion.
That doesn't mean COMLEX is trickier in a cheap way. It means pattern recognition alone won't carry the item.
Every word doesn't matter equally
Students sometimes hear that COMLEX stems are full of fluff. I don't think that's the best way to read them. Some details are noise, yes, but the better interpretation is this: COMLEX often includes clues from different reasoning systems in the same stem.
A line about recent grief may matter for ethics. A line about upper thoracic tissue texture changes may matter for autonomics. A line about body position may matter for a musculoskeletal diagnosis. The issue isn't that the stem is bloated. The issue is that students read everything through one lens.
For students cross-referencing what overlaps with Step content, a concise USMLE content outline can be useful, but you still need a separate COMLEX reading strategy.
The biggest mistake
The biggest mistake is studying COMLEX as “USMLE plus some OMM.” That framing leads students to tack osteopathic review onto the end of their prep instead of weaving it into every clinical system.
If you do that, you'll know facts but miss the exam's logic. COMLEX rewards integration. That's the key difference.
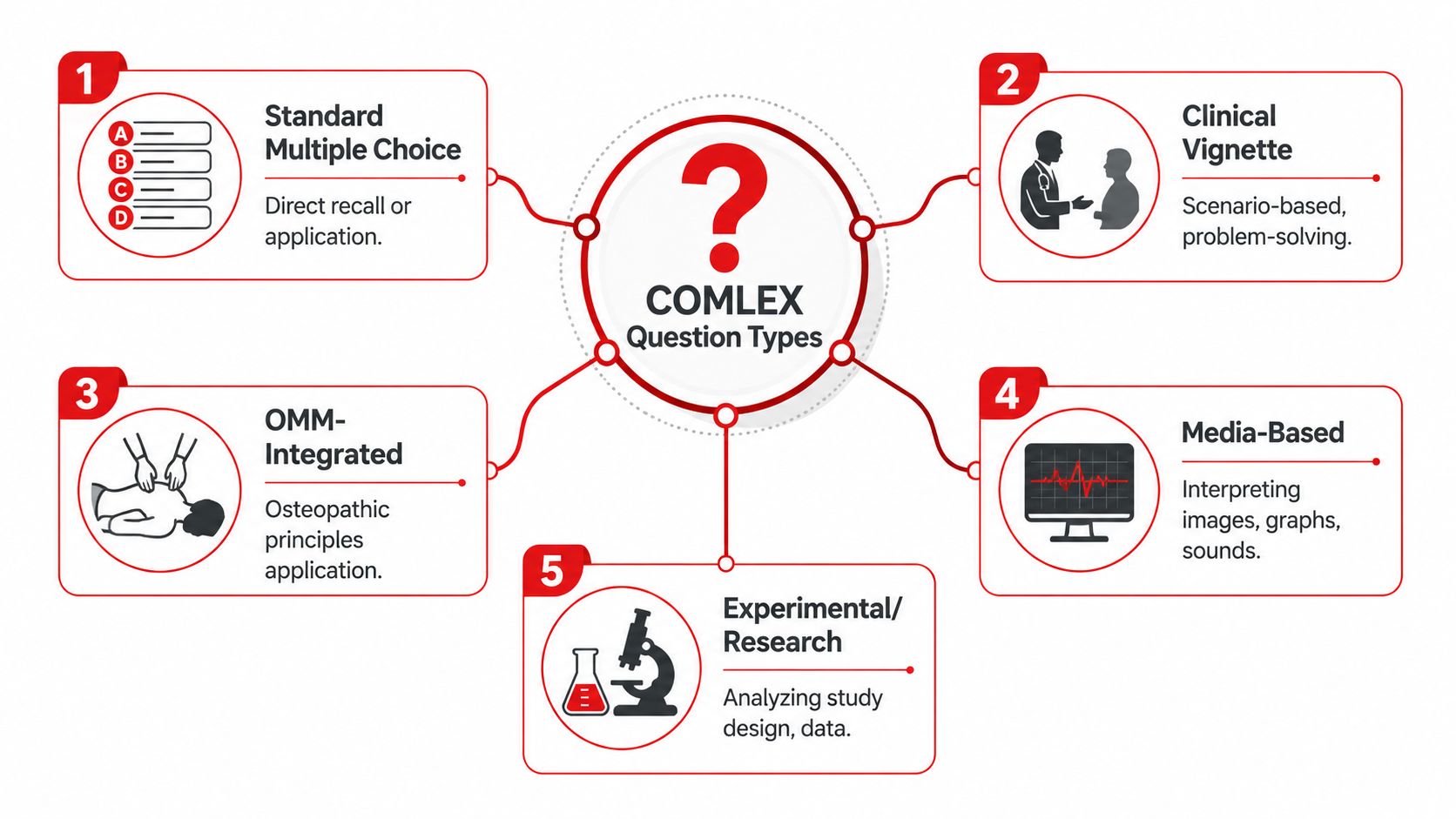
The 5 Main Types of COMLEX Questions to Master
You don't want to read every item from scratch on test day. You want to identify the type quickly so your brain uses the right approach.
As of May 2026, the exam uses 320 questions and includes audio-visual items alongside standard multiple-choice questions, with forward-only navigation so you can't return to an earlier section after leaving it, according to this overview of the updated format. That makes question-type recognition important immediately, not later in review.
Standard clinical vignettes
These are the bread-and-butter items. They look most familiar if you've used UWorld, AMBOSS, or classroom-style Qbanks.
Your job is to identify the disease process, mechanism, or next inference from standard medical data. The trap is assuming that because the stem looks standard, the answer choices will stay standard.
Pure OMM questions
These ask directly about osteopathic principles, diagnosis, or treatment. You'll often see topics like viscerosomatics, Chapman points, sacral mechanics, cranial concepts, rib dysfunctions, or treatment positioning.
These are usually missed for one of two reasons:
- Students memorize names but not patterns
- Students know the diagnosis but not the setup or implication
OMM-integrated vignettes
This is the category that causes the most frustration.
The stem starts like a regular pathology or physiology item. Then it adds structural findings or asks for the answer that best incorporates osteopathic reasoning into the case. Students who keep OMM in a separate mental folder often miss these.
For students looking for targeted resources, a focused list of COMLEX practice questions and study resources for DO students can help, but you still need to classify these stems correctly while you practice.
If the question includes both disease clues and body mechanics clues, assume COMLEX wants both.
Audio and visual questions
These require you to process images, sounds, or other media alongside the text.
Examples include:
- Heart or lung sounds
- ECGs
- X-rays or cross-sectional imaging
- Rashes or pathology images
- Short media exhibits paired with a clinical vignette
These questions are less about isolated recognition than about synthesis. Don't just identify the image. Tie it back to the clinical question being asked.
Professionalism, ethics, and biostats
These are easy to underestimate because students assume they can “reason them out.” Sometimes you can. Often the challenge is choosing the answer that is not merely acceptable but best aligned with exam framing.
In these items, slow down. Look for the option that is most patient-centered, most appropriate to role, or most methodologically sound. COMLEX often rewards mature judgment rather than fast instinct.
Sample Questions with Annotated Walkthroughs
The fastest way to improve on COMLEX Step 1 questions is to watch the reasoning process in slow motion.
Sample case 1
A patient presents with right upper quadrant pain after fatty meals, nausea, and tenderness under the right costal margin. The stem also mentions tissue texture changes in the mid-thoracic region. The question asks which osteopathic finding is most likely associated with this presentation.
You may think, “This is gallbladder disease.” Good. But don't stop there.
Step 1 read the stem in two passes
First pass, identify the core disease. This sounds like biliary pathology.
Second pass, ask what the osteopathic overlay is. The stem didn't include the thoracic finding by accident. It's redirecting you away from pure diagnosis and toward autonomic or viscerosomatic reasoning.
Step 2 predict before looking at options
Before the answer choices, say to yourself: “This is likely asking for the viscerosomatic region connected to hepatobiliary pathology.”
That protects you from distractors. If you go straight to the options, you'll often get pulled toward treatments or findings that are medically adjacent but not what the question is asking.
Step 3 test each answer choice by role
When reviewing options, ask what kind of answer each one is.
- Is this a disease fact
- Is this an OMM finding
- Is this a treatment technique
- Is this a management step
Many COMLEX misses happen because students compare options by topic instead of by role. If the stem asks for an associated osteopathic finding, then the “best antibiotic,” “best imaging,” or “best management” options are bait, even if they are medically sensible in the right context.
A COMLEX answer can be true and still be wrong because it answers the wrong question.
Sample case 2
A student gets this stem: a young patient has fever, sore throat, posterior cervical lymphadenopathy, and fatigue. The question asks which complication is most important to counsel the patient about. One answer choice is a classic microbiology association. Another is a practical clinical risk related to the disease course.
COMLEX distractor logic becomes clearly apparent.
What tempts students
The student recognizes infectious mononucleosis and then latches onto the answer choice that feels most “Step 1-ish,” usually a mechanistic or virology-flavored association.
But if the stem asks about counseling, the frame has changed. COMLEX wants the answer that best fits patient care and applied judgment.
The better internal monologue
Try this on every question:
- What is the diagnosis
- What exact task is being asked
- Which answer lives in that task frame
That third question is the one many people skip.
Here's a quick way to annotate your own review:
| Stem detail | What it tells you |
|---|---|
| Fever, fatigue, posterior cervical nodes | Likely infectious mononucleosis |
| Asking about counseling | This is not just a diagnosis question |
| Complication emphasis | Think patient safety and applied management |
If the best answer choice is the one tied to practical counseling and avoiding harm, that's the one COMLEX will usually favor over a more abstract science fact.
How to practice this skill
Write brief notes after missed questions in this format:
- I knew
- I missed
- The question was really testing
- The distractor that trapped me was
- Next time I'll look for
That review style is much more useful than writing, “Need to review mono” or “Need more OMM.”
A lot of students also learn this process better by hearing someone verbalize it. This walkthrough format is worth watching and then imitating in your own reviews:
The repeatable pattern
When you strip away the details, the expert approach is simple:
- Name the medical problem
- Identify whether there's an osteopathic overlay
- Determine the task the question is assigning
- Eliminate answers that belong to the wrong task
- Choose the one best answer, not the first true statement
That's how you turn COMLEX Step 1 questions from “weird” into predictable.
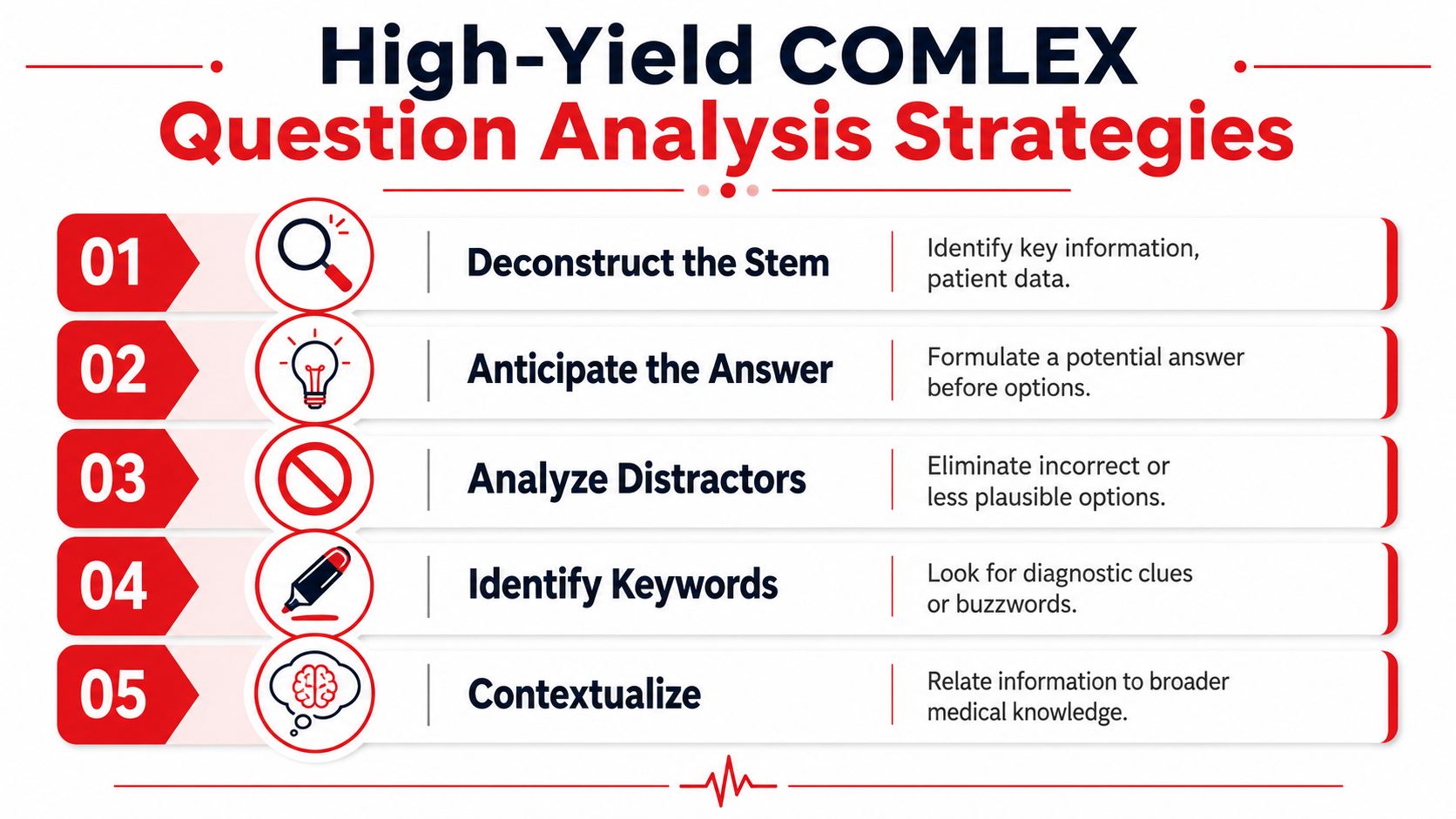
High-Yield Strategies for Analyzing Any COMLEX Question
The most useful COMLEX strategy isn't “do more questions.” It's learning how to read one question correctly the first time.
A major problem in prep is that even students doing 6,000+ practice questions still struggle with OMM-integrated stems because many Qbanks treat OMM and pathophysiology as separate silos. The same discussion points out that guides rarely explain the distractor logic behind items where both a USMLE-style and COMLEX-style answer look plausible, even though COMLEX enforces a one best answer rule, as described in this video discussion on COMLEX question logic.
Use the osteopathic overlay check
When you finish reading the stem, ask one forced question:
Is there an osteopathic overlay here?
That overlay might be:
- Structural findings
- Autonomic clues
- A treatment contraindication or indication
- A body-region relationship
- A patient positioning clue
- A palpatory or mechanical description
If you don't actively ask this, you'll often default to standard pathology reasoning and miss the point.
Separate task from topic
A question about pneumonia can still be asking about ethics. A question about gallbladder disease can still be asking about viscerosomatics. A question about mono can still be asking about counseling.
That's why I tell students to label the task before they pick an answer:
| If the task is… | Then prioritize… |
|---|---|
| Diagnosis | Best-fitting disease process |
| Mechanism | Physiology or pathology link |
| Associated finding | Linked exam, autonomic, or structural clue |
| Treatment | What is indicated or contraindicated |
| Counseling or ethics | Patient-centered, role-appropriate action |
Students who improve fastest usually get better at this distinction, not just at memorizing more content.
Analyze distractors by why they're tempting
A strong COMLEX distractor is rarely random. It usually falls into one of these patterns:
- Correct diagnosis, wrong task
- Reasonable medicine, wrong osteopathic frame
- Partially true statement, but not the best answer
- An answer that would fit another exam better than this one
When you review a miss, don't just ask why the right answer was right. Ask why the wrong one attracted you.
The distractor teaches you more about your test-taking than the correct answer does.
Expect application over recall
On some question types, especially professionalism, ethics, and data interpretation, simple memorization won't carry you. The exam increasingly rewards applied judgment. That means you should practice saying, “What would the most appropriate physician do here?” instead of “Which fact do I remember?”
For test-day discipline, this is the same skill students use to improve medical test-taking performance. You're not just learning medicine. You're learning how to classify and solve a specific style of prompt under pressure.
Building Your Personalized Practice Plan
A good COMLEX practice plan doesn't just accumulate questions. It trains pattern recognition, integration, and review quality.
One discussion of high-yield COMLEX prep notes that 10,000 unique practice questions may represent the threshold for the highest scores, while also pointing out that students still lack clear ways to separate COMLEX-specific difficulty from USMLE-style difficulty inside shared Qbanks, according to this discussion of COMLEX high-yield preparation. That's exactly why pure volume isn't enough.
What to do each week
Build your prep around three parallel tracks:
- Mixed timed blocks so you learn to switch between pathology, OMM, ethics, and media items without warning.
- Deep review where you classify every miss as knowledge gap, format mismatch, pacing error, or distractor trap.
- Targeted repair using resources like TrueLearn, COMBANK, COMQUEST, UWorld, AMBOSS, Savarese, class OMM notes, and official-style self-assessments.
If your review notes keep showing “I knew the disease but missed the osteopathic layer,” that's not a memorization issue. It's a reasoning pattern issue.
How to know your plan isn't working
A lot of students stay stuck because they respond to every bad block the same way. They just do more questions. That helps only if the problem is exposure.
Your current approach probably needs adjustment if:
- Your misses keep clustering around OMM-integrated stems
- You narrow to two answers but keep choosing the more generic one
- Your score plateaus despite heavy question volume
- You feel like COMLEX questions are unpredictable even after lots of practice
Those are signs that your issue is interpretation, not effort.
Quality beats blind repetition
You don't need every review session to be long. You do need it to be honest.
A student who does fewer questions but writes down recurring mistake patterns usually improves faster than a student who burns through block after block without identifying why the same trap keeps working. COMLEX rewards strategic repetition, not mindless repetition.
If you're putting in the hours but still feel stuck on OMM-integrated reasoning, COMLEX-specific distractors, or test-taking strategy, Ace Med Boards can help. Their one-on-one tutoring is built for exactly this kind of problem: turning confusing question blocks into clear patterns, tightening your reasoning, and helping you approach COMLEX with a plan that matches the exam.