You're probably reading this between admissions, after sign-out, or during the small window where you meant to eat and somehow ended up searching for USMLE Step 3 study material instead. That's normal. Step 3 catches almost everyone at a bad time. You're working, you're tired, and the internet keeps giving you either overbuilt study plans or vague advice like “just do questions.”
Here's the blunt version. You do not need every resource. You need a tight plan, the right materials, and enough discipline to stop resource-hopping. Step 3 rewards efficient prep far more than heroic prep. If you've already made it through medical school and earlier boards, you have the base. What you need now is targeted execution.
The biggest mistake I see is treating every test taker the same. A busy U.S. resident on wards does not need the same setup as an IMG trying to close gaps in U.S.-specific management, ethics, and practice style. Your background changes which materials will help you.
Decoding Your USMLE Step 3 Study Plan
You finish a long shift, open your laptop, and suddenly Step 3 feels bigger than it should. Ten browser tabs. Three Reddit threads. Five people telling you five different timelines. Ignore the noise. Your study plan should fit your actual life and your actual gaps, not some generic template built for a stranger with unlimited time.
Start there. A U.S. resident trying to pass efficiently while working full-time needs a different setup than an IMG who also needs more repetition in U.S.-style management, ethics, and care coordination. That difference matters. It changes how much time you need, how heavily you should weight question review versus CCS, and how aggressive your schedule can be.
Keep the structure simple. One main question bank. One CCS resource. One way to measure whether you are improving. If you keep collecting tools, you will confuse activity with progress.
For most residents, a part-time plan built over several weeks works better than a packed sprint because it survives call, clinic, and post-call fatigue. If you do have true dedicated time, you can compress the schedule. The rule is simple. Match the plan to your calendar, then match your materials to your background.
Build around the week you actually live
Write a plan for your worst week, not your best one.
Use a schedule like this:
- Workdays: 15 to 25 questions, focused review, and one CCS case if you still have enough concentration
- Lighter days: bigger question blocks, notebook review, and extra CCS reps
- Protected days off: self-assessments, missed-question review, and system cleanup
That is how you stay consistent. A study plan that only works on elective is useless.
If you want a more detailed framework for turning these principles into daily execution, this step-by-step guide on how to pass USMLE Step 3 is a practical reference.
Know what your plan is supposed to do
Step 3 rewards clinical judgment under pressure. It also rewards clean CCS execution. Your plan should train both from day one.
That means your study materials need to do three jobs:
- Expose weak spots in management and next-step thinking
- Build speed and accuracy with CCS orders and timing
- Show you whether your score is moving
Everything else is secondary.
Here's the mistake I see all the time. Residents underestimate CCS because they feel comfortable clinically. IMGs sometimes over-focus on content review and delay mixed question practice too long. Both groups lose points for predictable reasons. Residents drop easy CCS points through sloppy software habits. IMGs miss management patterns, preventive care details, and test-writer logic that only improve through repeated question review.
So build your plan with a purpose. If your baseline knowledge is solid and your time is short, keep it tight and question-heavy. If your foundation needs work, give yourself a longer runway and more review time. Generic Step 3 advice misses that distinction. You should not.
Your Essential USMLE Step 3 Study Material Toolkit
You finish a long call day, open ten tabs, and suddenly your Step 3 plan is a mess. One person says buy three qbanks. Another says read a review book cover to cover. Someone else says CCS can wait until the last week. That advice wastes time.
Your toolkit should stay small and purposeful. The right mix depends on who you are and how much runway you have. A busy U.S. resident usually needs a tight, question-first setup. An IMG with a longer timeline may need the same core tools plus a structured review layer to close practice-pattern gaps.
Start with the visual overview below.
Your core materials
UWorld Step 3 should be the center of your prep. It does the job Step 3 prep needs to do. It exposes weak management patterns, forces next-step thinking, and gives you enough repetition to see whether your mistakes are random or predictable.
Use it actively. Tag misses. Review why the wrong choices were wrong. Track recurring themes like preventive care, OB triage, inpatient management, ethics, and biostats. If you finish blocks and only look at your percentage, you are wasting the best resource in your stack.
A huge library is not required. Four tools used correctly are sufficient.
| Resource | What it's for | My recommendation |
|---|---|---|
| UWorld Step 3 QBank | Core MCQ prep and weakness identification | Make this your main study engine |
| Official Primum software | Learning the real CCS interface | Download it early and practice in the real format |
| CCS case platform | Repetition, timing, order sequencing | Use regularly, not just near test day |
| NBME self-assessments | Benchmarking before test day | Use after you've built enough question volume to get a meaningful read |
| Free 137 | Final style check and confidence pass | Save for the end |
Where a review book fits
A review book is optional. For many U.S. residents, it adds very little because the deficit is execution, not raw content. For IMGs or anyone who has been away from broad clinical review, a concise reference can help organize scattered topics and clean up weak areas between question blocks.
If you want a short reference to support your qbank work, this First Aid guide for USMLE Step 3 planning is a reasonable place to decide whether a review book fits your study style.
CCS needs its own lane
CCS is a separate skill. Strong clinical knowledge helps, but it does not automatically give you points if your orders are late, your timing is sloppy, or you are unfamiliar with the software. I have seen good test takers lose easy points here because they treated CCS like an afterthought.
Use the official Primum software early so the interface stops feeling awkward. Pair that with a CCS case resource for repetition. Your goal is simple. Get fast at initial orders, know when to advance the clock, and stop missing basic inpatient and outpatient cleanup steps like monitoring, counseling, disposition, and preventive follow-up.
If your timeline is short, keep the toolkit even tighter:
- UWorld
- Official Primum
- One CCS case resource
- One self-assessment
If your timeline is longer, especially for an IMG, add a concise review layer only if your blocks show broad knowledge gaps.
That is enough for almost everyone.
Use fewer resources. Use them harder.
Choosing Your Study Path Resident vs IMG
You and a co-intern can sit for the same Step 3 and need different prep. One of you is a U.S. resident who sees admissions, discharge planning, and preventive care every week but studies in short, tired bursts. The other is an IMG with strong medical knowledge who keeps losing points on U.S. management patterns, ethics wording, and what the exam expects you to do next. If you use the same plan, one of you wastes time.

If you're a U.S. resident
Your main problem is usually not medical knowledge. It is inconsistency.
You already think in the clinical style Step 3 rewards. You hear treatment plans on rounds, you see common inpatient problems repeatedly, and you have a decent feel for what matters in real patient care. What hurts residents is scattered studying, underestimating CCS, and assuming daily work automatically turns into exam points.
Build your USMLE Step 3 study material around efficiency:
- Primary tool: UWorld
- Reference support: AMBOSS for quick clarification when a concept is particularly weak
- Priority gaps: CCS workflow, biostats, ethics, and pacing across both test days
Do not build a resident plan around heavy reading. Finish question blocks, review them hard, and fix the misses that keep repeating. Your clinical exposure already covers a lot of the foundation. Your job is to translate it into board-style answers under time pressure.
If you're an IMG
Your main problem is usually not effort. It is alignment with the U.S. exam.
Many IMGs know the medicine well and still miss Step 3 questions because the test rewards U.S.-specific preventive care, guideline-based management, communication style, and order sequencing. That is why broad reading alone often feels productive but does not move scores enough.
Your prep should be more targeted than a resident's plan:
- Primary tool: UWorld, used aggressively to identify recurring misses
- Second layer: focused review of U.S. practice patterns, ethics, screening, vaccination, and disposition decisions
- Priority gaps: outpatient management, next-best-step logic, and CCS habits that reflect U.S. workflow
If that sounds familiar, read this IMG guide to U.S. training pathways and planning to place Step 3 in the bigger picture.
One warning matters here. Covering more pages does not fix a narrow mismatch. If you keep missing the same U.S.-style management questions, stop reading broadly and start drilling that exact weakness.
A side-by-side decision guide
| Background | Main strength | Main risk | Better material strategy |
|---|---|---|---|
| U.S. resident | Daily clinical exposure and familiarity with common management decisions | Irregular study time, fatigue, weak CCS execution | QBank-first plan with selective concept lookup |
| IMG | Strong base knowledge and high motivation | Misses tied to U.S.-specific management, ethics, and preventive care | QBank-first plan plus focused review of U.S. guidelines and repeated weak themes |
What I'd tell each group directly
For residents, stop collecting resources. Finish one plan.
For IMGs, stop treating every miss like a content deficit. A lot of your lost points come from exam framing, not lack of intelligence.
Same exam, different pressure points. Build your study path around the one you have.
A Sample 6-Week USMLE Step 3 Study Schedule
You get home after sign-out, open your laptop, and waste 20 minutes deciding what to study. That is how Step 3 prep falls apart. A good schedule removes those decisions. You should know what to do on a tired Tuesday, a post-call afternoon, and a free Sunday.
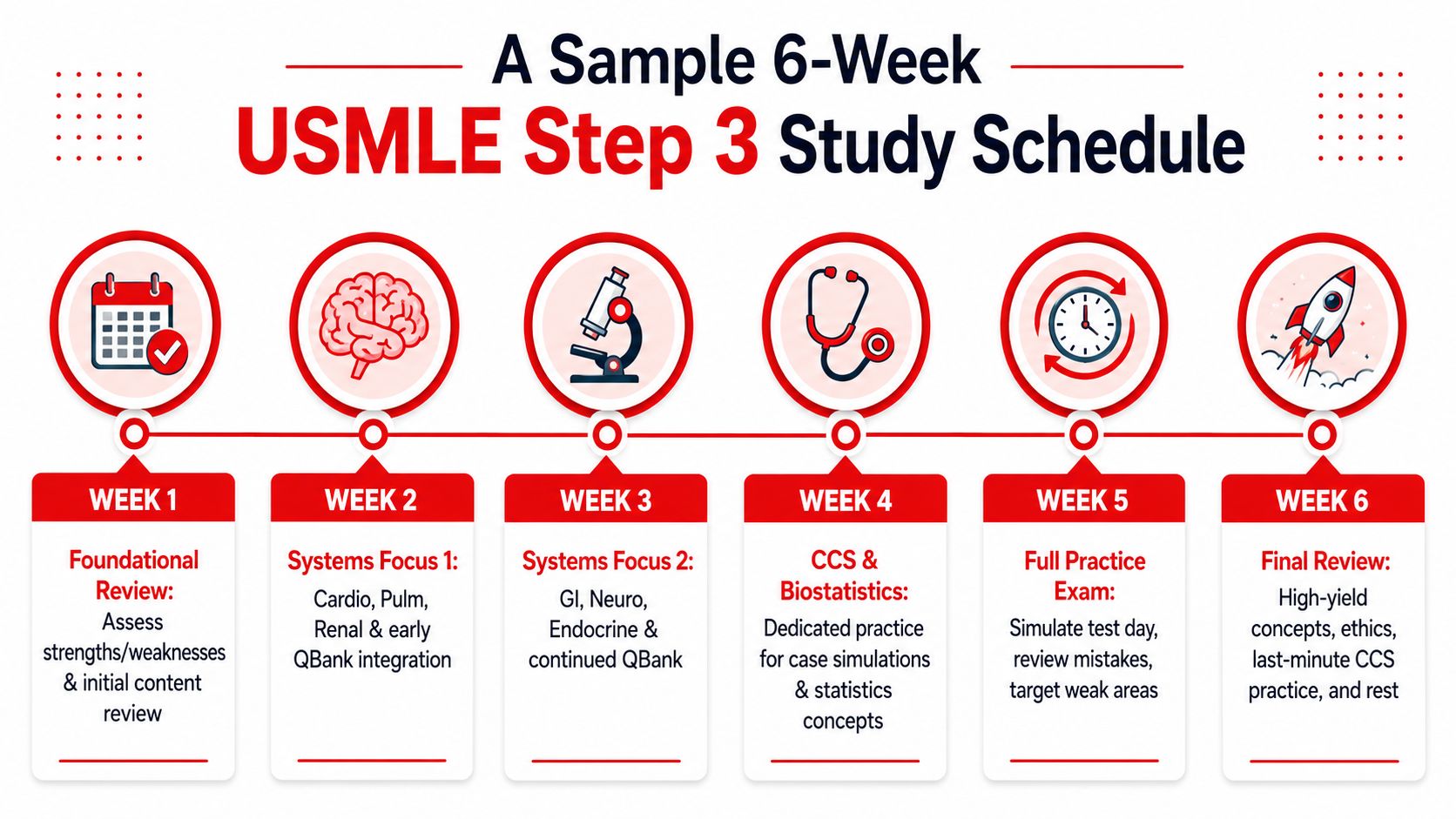
This 6-week plan works because it fits real clinical schedules and leaves room to adjust based on who you are. Residents usually need tighter time control and more accountability. IMGs often need a little more deliberate review of U.S.-style management and preventive care questions inside the same schedule. Same framework. Different points of emphasis.
Use one qbank, do CCS throughout, and review mistakes hard. Everything else is optional.
Weeks 1 and 2
Start by building control. Do not chase random mixed blocks yet if your misses are still clustered. Early prep is for identifying patterns, cleaning up weak systems, and setting a daily rhythm you can repeat.
Use this structure:
- Questions: 30 to 40 on most study days
- Mode: Tutor mode or focused blocks by subject
- CCS: 1 to 2 cases a day
- Review: Write down why you missed the question. Knowledge gap, management error, or careless read
Residents should bias these first two weeks toward efficiency. Hit weaker areas fast and move on. IMGs should spend extra review time on outpatient follow-up, screening, ethics, and next-best-step decisions, because those misses often come from exam framing, not lack of medical knowledge.
If you want a model calendar you can plug into your rotation schedule, use this 6-week Step 3 study schedule template. For retention, build a short review loop instead of rereading explanations. This article on optimizing study time with spaced repetition gives a practical framework you can apply to missed questions and CCS checklists.
Weeks 3 and 4
Now increase pressure.
Shift toward timed sets on your better days. Keep some focused review if one subject is still dragging your score down, but your prep should start looking more like the actual exam. You need practice switching from medicine to peds to OB/GYN without a warm-up.
Middle-phase priorities:
- Increase question volume on lighter days
- Do more mixed, timed blocks
- Track repeat misses in a simple error log
- Keep CCS daily, even if it is only one case
- Review biostats and ethics every week instead of saving them for the end
Take a self-assessment near the end of this stretch if you have one available. Use it to spot patterns. If your score drops because of broad weakness, you need more question volume and review. If it drops because of a few repeated categories, fix those directly.
A weak practice score is useful if you respond to it.
Weeks 5 and 6
These final two weeks are for execution. Stop tinkering with resources. Stop making new color-coded plans. Your job now is to perform under timed conditions and tighten the mistakes that still cost easy points.
Focus on four things:
- Mixed timed blocks: build stamina and improve switching between subjects
- CCS repetition: fix ordering mistakes, missed disposition, and poor time advancement
- Targeted review: revisit incorrects and notes from your error log
- Practice exam work: use a formal checkpoint if it fits your plan
If you are a resident with very limited time, protect questions and CCS first. If you are an IMG with a bit more flexibility, use the extra hour for targeted review of U.S.-specific management patterns, not for adding another resource.
A weekly rhythm that survives residency
| Day type | What to do |
|---|---|
| Busy call day | 10 to 20 questions, quick review, one CCS if you still have focus |
| Normal weekday | One main question block, full explanation review, one CCS case |
| Weekend or lighter day | Higher-volume question work, 2 to 4 CCS cases, cleanup of repeated weak areas |
Consistency wins here. A plain plan you follow for six weeks beats an ambitious plan you abandon after four days.
Mastering CCS Cases and High-Yield Topics
If you want the fastest score improvement per hour, spend serious effort on CCS, biostatistics, and ethics. A lot of residents delay these because they feel awkward or annoying. That's exactly why they remain point-rich.
Biostatistics and ethics are disproportionately high-yield on Step 3, and examinees improve by mastering odds ratios, relative risks, and confidence intervals. Common formats include drug advertisement interpretation and study abstract analysis, as discussed in this Step 3 high-yield Reddit guide. Don't leave these for the final weekend.
How to approach CCS without overcomplicating it
Most CCS mistakes fall into a few buckets:
- You delay urgent interventions
- You forget disposition and follow-up
- You order things in the wrong sequence
- You know the medicine but fight the interface
The cure is repetition with feedback. Do cases often enough that the workflow becomes automatic. Open the case, stabilize if needed, order focused diagnostics, treat what can't wait, advance the clock appropriately, reassess, then close cleanly.
A dedicated guide to Step 3 CCS cases and computer simulations can help if this remains your least comfortable area.
Don't practice CCS to “see more cases.” Practice CCS to build a reflexive order sequence.
A quick framework for non-clinical questions
For drug ads and abstract questions, stop trying to read every word first. Start with the question stem. Figure out what they want from you, then go hunting for the relevant data. That cuts down panic and wasted time.
Use this mental checklist:
- What's the task? Calculate, interpret, identify bias, or compare outcomes.
- What metric matters? Odds ratio, relative risk, confidence interval, study type.
- What can you ignore? Most of the fluff in the ad or abstract.
- What's the safest answer under pressure? The one supported directly by the data provided.
If retention is the issue, build a small review loop instead of rereading the same notes. I like optimizing study time with spaced repetition for formulas, ethics distinctions, and recurring management rules because it keeps small facts from evaporating between shifts.
What deserves priority in the final stretch
Focus hard on these:
- Biostatistics formulas and interpretation
- Ethics, communication, and patient safety
- Drug ad questions
- Study abstracts
- CCS rhythm and common order patterns
The residents who struggle most are often solid clinically but sloppy in these “board-ish” areas. Fix that and your score usually follows.
When to Consider a USMLE Step 3 Tutor
You're five or six weeks out. You're studying after call, doing blocks when you can, and still missing questions for reasons you can't explain. At that point, more effort is not the answer. Better feedback is.
The right reasons to get help
A tutor makes sense when your weak points are specific and persistent. If you keep missing the same management questions, freezing on exam strategy, or wasting hours on review that never changes your performance, self-study has stopped being efficient.
That applies to different people for different reasons. A U.S. resident usually needs efficiency, accountability, and fast correction of bad test habits. An IMG often needs that plus adaptation to U.S. exam logic, ethics framing, and the management style Step 3 rewards. Generic advice misses that difference. Good tutoring should not.
Consider getting help if any of these fit:
- You have recurring knowledge gaps: The same topics keep showing up in your misses, and review is not fixing them.
- You're an IMG adjusting to the exam style: You need direct coaching on how Step 3 asks questions and what kind of answer it wants.
- You underperform on standardized tests: Your issue may be pacing, question interpretation, or second-guessing, not just content.
- You already failed Step 3: You need a new system, not more random question blocks.
- Your schedule is crushing your consistency: If residency leaves you with scattered study time, outside structure can keep you from losing weeks.
What a tutor should actually do
A good Step 3 tutor should diagnose the problem fast. They should review your misses, find patterns, and tell you what to stop doing. They should also tailor the plan to your timeline. A resident with four weeks needs a triage plan. An IMG with ten weeks may need more work on exam style and decision-making patterns.
They also need to be practical. That means tightening your question approach, cleaning up pacing mistakes, and making sure your study plan matches your background instead of copying a forum post from someone in a completely different situation.
Ace Med Boards is one option for one-on-one Step tutoring with a personalized approach to scheduling, question review, and targeted weak-area work. That kind of support is useful if you need structure, direct feedback, and a plan built around your actual constraints.
If you're six weeks out and still don't know why you're missing questions, the problem is not motivation. The problem is lack of accurate feedback.
Do not wait until you've burned two more weeks and your confidence drops. If your current plan is not turning study time into better performance, get help early enough for it to matter.