You've probably heard some version of this already: “Get some shadowing.” The problem is that nobody says what “some” means, how to get it without awkwardly cold-emailing half your city, or how to make those hours matter once you're there.
That uncertainty creates a lot of unnecessary stress. Students either underdo it because they don't know where to start, or overdo it because they think admissions wants a giant stack of hours with no clear purpose behind them.
Medical student shadowing works better when we stop treating it like a scavenger hunt. The strongest use of shadowing is twofold. It helps you show admissions that you understand the day-to-day reality of medicine, and it sharpens the habit that matters on exams and in clinics alike: noticing how physicians move from symptoms to differential, testing, and management. That second part is the piece most guides miss. If you use shadowing well, it becomes an early form of clinical reasoning practice.
Why Shadowing Is More Than Just an Application Checkbox
You finish a shadowing day, write down four hours, and realize you remember almost nothing except the specialty and a few room numbers. That is the version of shadowing that feels like a box to check, and it usually stays a weak experience on both applications and later clinical training.
Useful shadowing does more than confirm that you spent time near physicians. It shows you how medicine is practiced under time pressure, incomplete information, and competing patient priorities. A lecture gives you a clean presentation of chest pain or fatigue. Clinic gives you a patient with vague symptoms, medication nonadherence, transportation problems, and only fifteen minutes to sort out what matters first.
That difference matters early.
Admissions committees want evidence that you understand the profession beyond the idea of it. Shadowing helps establish that. It also gives you an early view of how physicians build a differential, test a hypothesis, and adjust a plan when new details change the picture. Those are the same habits you will need on rotations, on shelf exams, and later on USMLE or COMLEX question sets.
I wish more students were told this upfront. If you watch carefully, shadowing becomes early clinical reasoning practice.
For example, notice what happens when an attending asks one extra question about timing, associated symptoms, or medication use and suddenly the differential shifts. That is not just interesting bedside conversation. It is the practical application of the board-style move from broad complaint to discriminating detail. Students who train themselves to spot those pivots tend to learn disease scripts faster because they are seeing how findings change probability, not just memorizing lists.
This is also why specialty choice matters less at the start than many students think. A half day in family medicine, internal medicine, pediatrics, or emergency medicine can all teach the same core skill. Watch how the physician frames the problem, identifies red flags, and decides what can wait versus what needs action now. If you are still looking for settings to observe, a practical list of physician shadowing opportunities near me can help you identify realistic starting points.
The students who get the most from shadowing are not the ones with the flashiest hour totals. They are the ones who can later say, with specifics, what they saw and how it changed their understanding of patient care.
That is the standard we should use. Shadowing should leave you with clearer judgment, stronger examples for applications, and a better eye for the clinical reasoning patterns that show up again when board prep gets serious.
Finding and Securing Meaningful Shadowing Opportunities
The hardest part of medical student shadowing is often the first yes. Students assume they need insider access. Usually, they need a cleaner process.
This roadmap works because it starts with warm options, then moves to professional outreach only after the easy wins are exhausted.

Start with people who can make a soft introduction
Your first asks shouldn't be random.
Reach out to:
- Pre-health advisors who keep lists of alumni and affiliated clinicians
- Science faculty who know physicians through research or community partnerships
- Current medical students who can tell you which departments are open to observers
- Family and family friends if they can make an introduction without putting pressure on the physician
A warm introduction doesn't guarantee a spot, but it lowers friction. Physicians are busy. Anything that makes your request feel legitimate and easy to process helps.
If you need a broader starting point, use a practical directory of physician shadowing opportunities near me to identify settings and specialties worth targeting.
Cold outreach works when it's specific
Most cold emails fail because they sound mass-sent, vague, or entitled. A good message is short, respectful, and easy to answer.
Include five things:
- Who you are. Your school, year, and basic training level.
- Why you're writing to them specifically. Their specialty, clinic type, patient population, or role.
- What you're asking for. Observation only, with flexible dates.
- Your awareness of logistics. You're willing to complete privacy forms, onboarding, or institutional requirements.
- A simple close. Ask whether they or their office coordinator would be the right contact.
Use a professional email, not a dramatic one
Don't oversell your passion. Don't give your life story. Don't say medicine has been your dream since childhood. Those lines aren't persuasive because they don't reduce work for the recipient.
What does help is showing that you understand shadowing is observational, that you respect patient privacy, and that you're flexible.
| Template Type | Subject Line | Email Body Snippet |
|---|---|---|
| Direct physician outreach | Shadowing request from [Your School] student interested in [Specialty] | Hello Dr. [Name], I'm a [year] student at [school] with an interest in [specialty]. I'm reaching out to ask whether you ever allow students to shadow in clinic or hospital settings. I'd be grateful for the chance to observe your workflow and learn more about the specialty. I'm happy to complete any required paperwork or training. |
| Coordinator-first outreach | Student observer request for Dr. [Name] | Hello [Coordinator Name], I'm a [year] student at [school] and hoped to learn whether Dr. [Name] accepts student observers. I'm interested in [specialty] and am looking for a brief observational experience. If there is a formal process through your office, I'd appreciate your guidance. |
| Alumni connection | Referred by [Mutual Contact] regarding shadowing opportunity | Hello Dr. [Name], [Mutual Contact] suggested I contact you. I'm a [year] student at [school] exploring [specialty], and I'd value the opportunity to shadow your practice if your schedule and institution allow. I understand clinic workflows are busy, so even a limited observational opportunity would be appreciated. |
| Follow-up email | Following up on shadowing request | Hello Dr. [Name], I wanted to briefly follow up on my earlier email regarding a possible shadowing opportunity. I know your schedule is demanding, so I completely understand if this isn't feasible. If there is someone else in your office I should contact, I'd be grateful for that direction. |
Keep your ask small. A physician is more likely to say yes to one half-day or one short block than to an open-ended request that sounds like a semester-long commitment.
Follow up once, then move on
A polite follow-up is appropriate. Repeated nudges aren't.
Use this rule:
- One initial email
- One brief follow-up
- Then redirect your energy elsewhere
Students often burn out because they keep waiting on nonresponses instead of building a small outreach pipeline. It's better to contact a manageable list of targeted physicians than to obsess over one dream mentor who never replies.
Choose settings that teach, not just impress
Students often chase glamorous specialties too early. That can backfire. You may get a narrower window into medicine than you would in a general clinic.
If you want a strong foundation, start with places where doctors explain decisions out loud and where you can see common complaints, medication management, preventive care, and follow-up. Primary care, internal medicine, and family medicine usually offer richer observation for beginners because the clinical reasoning is visible rather than hidden behind procedures.
That visibility matters later when you're trying to connect shadowing to board-style learning.
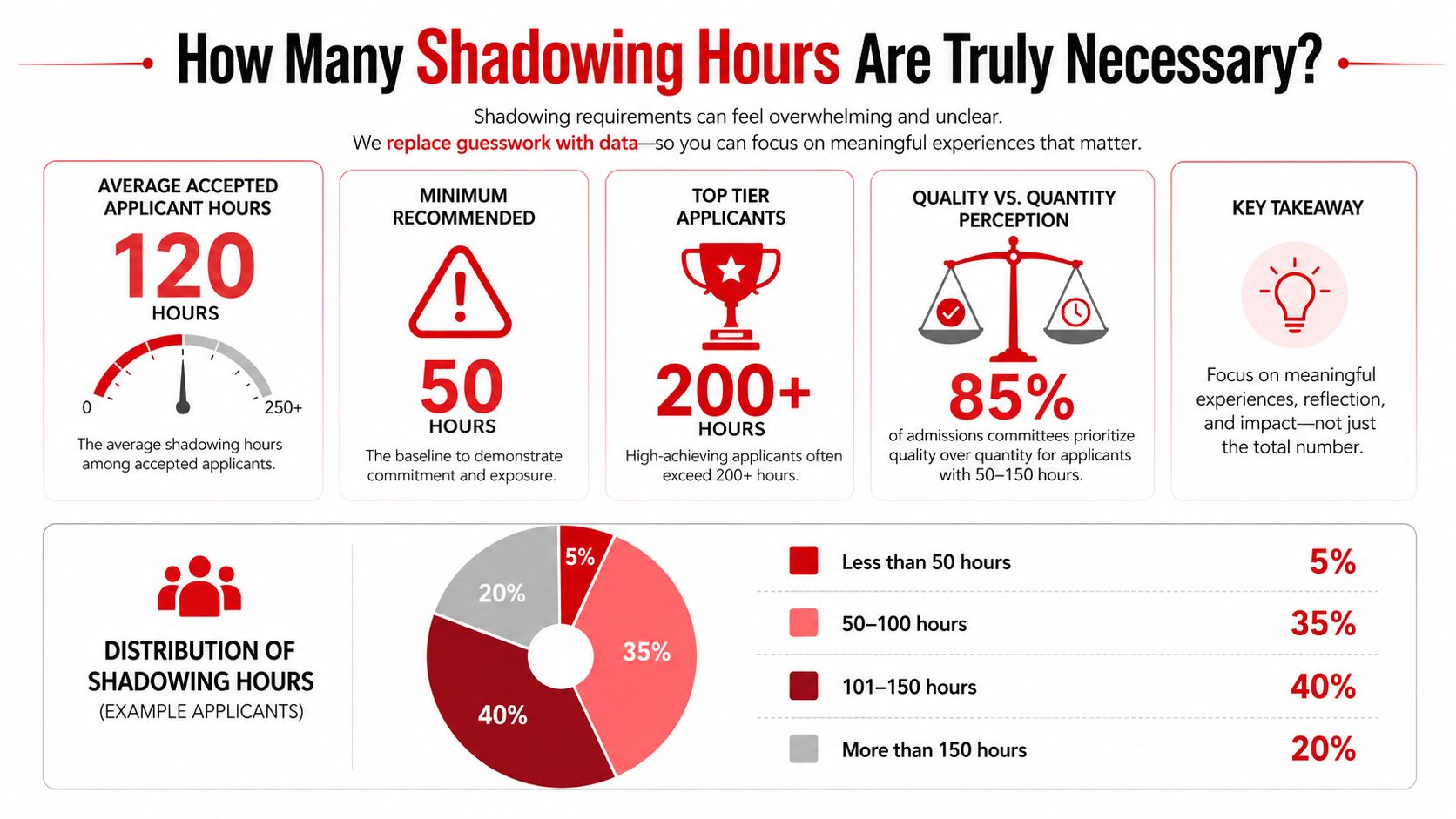
How Many Shadowing Hours Are Truly Necessary
A lot of students hit this point in the process with the same worry. Someone in a pre-med group chat says 150 hours is the minimum. Someone else claims every serious applicant has shadowed half a dozen specialists. Stress rises fast, and students start treating shadowing like a race instead of a learning tool.
The calmer answer is that you need enough hours to show sustained exposure to clinical medicine, enough variety to compare settings, and enough reflection to explain what you learned.
For accepted U.S. medical students, the median shadowing total is typically about 50 to 75 hours, with the interquartile range running from roughly 25 to 30 hours at the 25th percentile to 100 to 120 hours at the 75th percentile, based on a data review of matriculant shadowing hours. The same review notes that very few successful applicants report 400 to 500 hours of shadowing alone, and the 90th percentile often reaches only 200 to 250 hours.
That matters because shadowing competes with other parts of your development. Time spent chasing extra observational hours is time not spent on grades, service, research, paid clinical work, or recovery. I usually advise students to stop asking, “How high can I get the number?” and start asking, “Have I seen enough medicine to speak truthfully about the work?”
Aim for depth first, then contrast
A strong plan usually has one main home base and a small amount of contrast around it.
A data review on specialty breadth vs depth in admitted applicants found an optimal pattern of 60 to 80 total hours, with a central 40 to 120 hours range, and at least 30 to 40 hours in one primary specialty plus exposure to 3 to 5 different clinical environments.
That pattern makes sense from both an admissions and learning standpoint. Repeated time in one setting lets you see follow-up, workflow, diagnostic uncertainty, and how a physician adjusts a plan when the first idea is wrong. Shorter experiences in other settings give you comparison. You start to notice what changes between primary care, specialty clinic, inpatient service, and procedural environments.
That comparison is where shadowing starts helping with board-style thinking.
USMLE and COMLEX questions reward pattern recognition, differential diagnosis, and knowing which details matter most. Good shadowing can support those habits early. Watching an internist sort chest pain, fatigue, edema, or uncontrolled diabetes in real clinic gives context to the same problems you will later study in First Aid, UWorld, or COMBANK. You are not learning board content by osmosis, but you are building a mental framework for clinical reasoning.
A practical target looks like this:
- 30 to 40 hours in one core setting where you can follow the physician's thought process repeatedly
- 10 to 20 hours in one or two contrasting settings so you can compare pace, patient population, and decision-making
- Brief written reflection after each session focused on why a decision was made, not just what happened
If you want help generating better observations, keep a short list of questions to ask when shadowing a doctor and use them selectively at appropriate moments.
More hours help less after a point
The same source reports that applicants with 20 to 80 hours of shadowing had an acceptance rate of about 42%, nearly double the about 21% rate for those with fewer than 20 hours, with gains diminishing beyond 150 to 200 hours once GPA and MCAT are controlled, according to the same breadth-vs-depth analysis.
That is the trade-off. Early hours often change your application because they move you from minimal exposure to meaningful exposure. Later hours only help if they add new insight, stronger reflection, or a clearer understanding of patient care.
Students sometimes assume that a huge total proves commitment. Admissions readers usually care more about whether your experiences sound real. A student with 60 thoughtful hours can come across far better than a student with 220 hours and nothing to say beyond “I confirmed I like medicine.”
Hours alone are a weak metric
A better question is whether you can describe how physicians reason under uncertainty.
Can you explain why one complaint triggered a broad differential while another was managed conservatively? Did you notice how social factors changed a treatment plan? Did you see how pretest probability affected which test came next? Those are the observations that make your shadowing useful on applications and later in preclinical coursework.
Keep your target simple:
- one setting where you get repetition
- one or two settings that provide contrast
- enough exposure to explain what you learned about clinical reasoning, patient communication, and the day-to-day work of medicine
That is usually enough.
Preparing for Your First Day of Shadowing
Your first day doesn't require brilliance. It requires preparation, calm judgment, and basic professionalism.
Most awkward first days come from avoidable mistakes. Students show up underdressed or overdressed, forget paperwork, use their phones at bad moments, or arrive without any sense of the clinic they're entering. None of that helps you learn, and all of it is fixable.
Handle the paperwork before you arrive
Every institution has its own process. Don't assume you can walk into a clinic because a physician said yes.
Ask in advance about:
- Privacy training such as HIPAA modules or confidentiality agreements
- Occupational health requirements like immunization records or screening documentation
- Badge or visitor access rules for the site
- Dress expectations for clinic, hospital floors, or the operating room
If you're unclear, ask the office coordinator rather than guessing. Coordinators often know the practical rules better than anyone else.
Dress for the setting and stay unobtrusive
Business casual is usually the safest default unless the office tells you otherwise. Clean shoes matter more than stylish ones. You may stand longer than you expect.
Bring:
- A small notebook and pen for short observations and questions
- Photo identification if the site requires check-in
- A water bottle or snack if allowed and if the session is long
- A printed confirmation email if the institution is strict about access
Leave behind:
- Strong fragrances
- Large bags
- Anything that makes noise
- The habit of taking notes on your phone in patient areas
If you want a practical list of questions to ask when shadowing a doctor, prepare them before you arrive. The quality of your questions improves a lot when you're not improvising under pressure.
Know your role before the first patient enters
You are there to observe, not to perform. That sounds obvious, but it changes how you carry yourself.
Introduce yourself briefly if the physician wants you to. Step where you're told. Don't interrupt visits. Don't touch charts, equipment, or anything in a sterile field unless someone directly instructs you to do so.
Respectful silence is a skill. Students sometimes think they need to look engaged by filling space. In clinics, restraint often looks more professional than enthusiasm.
A strong first day is quiet competence. Show up early. Pay attention. Write down what you want to ask later. If you do those things well, the physician will usually open the door to more teaching on their own.
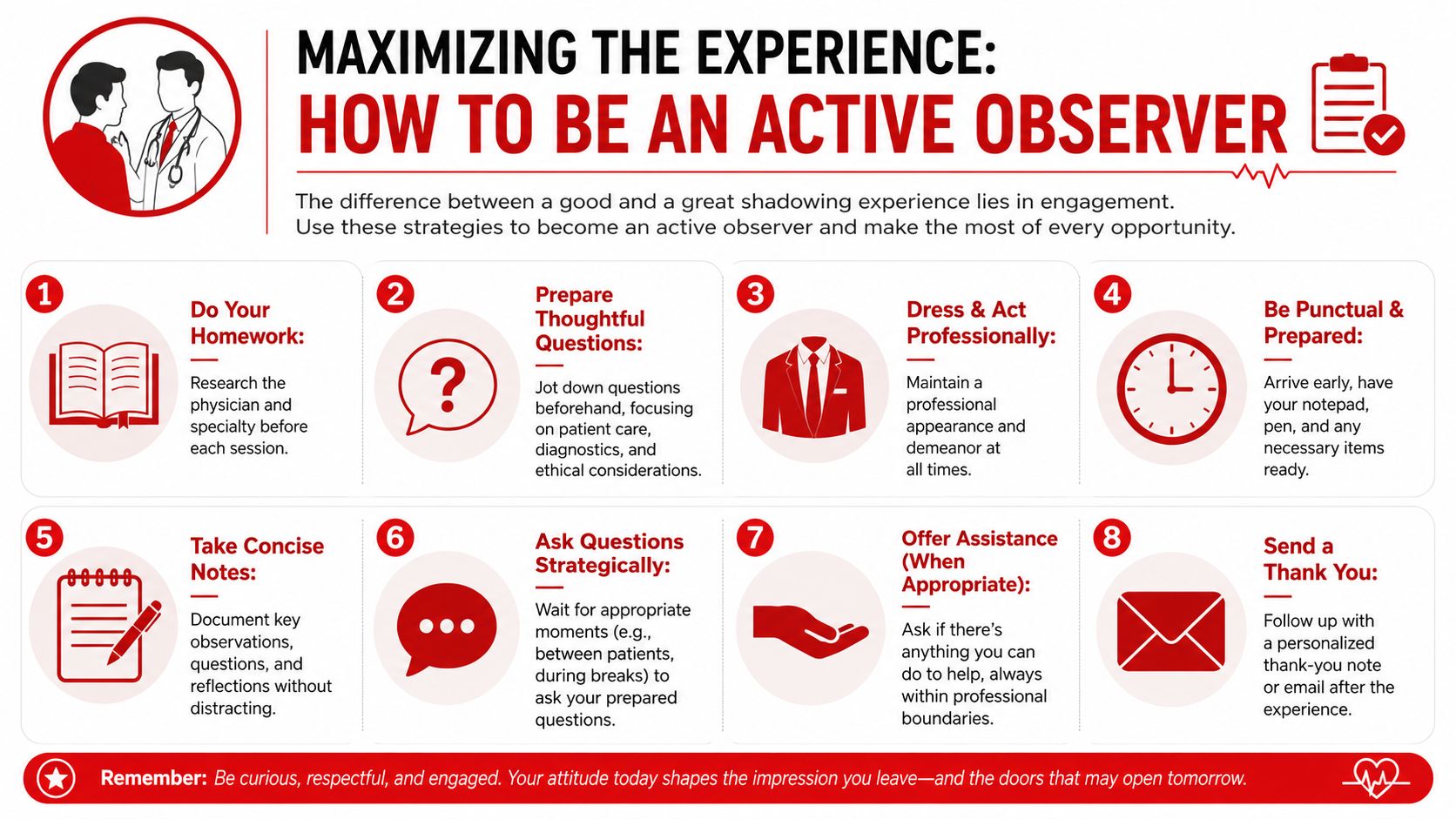
Maximizing the Experience How to Be an Active Observer
You are standing in the corner of a clinic room, trying to stay out of the way, and the physician changes the whole plan after hearing one extra sentence from the patient. That is the moment to study. Shadowing pays off when we learn to catch the reasoning behind the decision, not just the diagnosis at the end.
A memorable case can keep you interested. Clinical reasoning is what teaches you something. Watch for the chain: what clue mattered, what possibilities stayed on the table, what got ruled out, and why the physician chose to test, treat, reassure, or wait. That habit helps with applications because it gives you substance to write about. It also helps with boards because USMLE and COMLEX questions reward the same pattern recognition.
Watch the clinical reasoning sequence
Use a simple mental framework during each encounter:
- Chief concern
- Key history clues
- Focused exam or data points
- Differential narrowing
- Testing or treatment choice
- Patient counseling
This structure mirrors how good board questions are built. The stem gives you a complaint, then slips in one or two details that should change your differential or your next step. In clinic, you get to see that process happen in real time, including the uncertainty that question banks often compress.
Pay attention to pivots. If the physician changes course because of medication use, symptom timing, a red-flag review of systems answer, or a social factor like cost or transportation, make a note after the visit. Those are the details that build disease scripts. Over several sessions, you start seeing recurrent patterns instead of memorizing isolated facts.
Ask questions that reveal the physician's thought process
Students often default to specialty choice questions because they feel safe. Those have a place, but they should not be the main event if your goal is to learn medicine.
Better questions are specific and tied to a case:
- What part of the history pushed this diagnosis higher on your list?
- What were you most concerned about missing here?
- What finding would have changed your management?
- Why was watchful waiting reasonable in this case?
- What mistake do early learners make with presentations like this?
Timing matters as much as the question itself. Ask between patients, during a natural pause, or at the end of the session. In the room with a patient, silence and attention usually show better judgment than trying to sound insightful.
One practical rule helped me early on. If a question would interrupt patient trust, slow care, or force the physician to teach while multitasking, write it down and save it.
Turn shadowing into study material
Here, shadowing starts helping beyond applications.
After each session, write down four things:
- One common presenting symptom
- One short differential diagnosis pathway
- One management decision that surprised you
- One communication issue, such as low health literacy, adherence, cost, or fear
Then connect those notes to your coursework or board prep. If you are in preclinical training, match the case to your current system block and a related question-bank topic. If you are preparing for shelf exams or boards, convert the encounter into a short illness script with key positives, key negatives, and the decision point that changed management. A practical framework for active learning methods that improve retention can help you turn those observations into retrieval practice instead of passive review.
The trade-off is time. Detailed reflection after every session is ideal, but not always realistic. A focused five-minute note written the same day is far more useful than a perfect summary you never complete.
This walkthrough pairs well with the observation habits above:
Build reflections that show judgment
Strong reflection is concrete. “I confirmed I want to be a doctor” tells an admissions reader very little. “I watched a physician narrow a broad differential without overtesting, then explain the plan in language the patient could act on” shows that you noticed how medicine is practiced.
That same habit strengthens exam performance. Students improve when they stop treating medicine as a pile of disconnected facts and start organizing it around clues, decisions, and consequences. Shadowing can accelerate that shift if we treat each session like a live lesson in diagnostic reasoning rather than background exposure.
After the Shadowing Ends How to Follow Up and Log Hours
The last day of shadowing is not the end of the professional interaction. It's the point where you either preserve the relationship or let it fade.
Students often underestimate how much a good follow-up signals maturity. It tells the physician that you paid attention, that you respect their time, and that you know how to close a professional loop.
Send a thank-you that proves you were present
A thank-you email should be prompt and brief. The most effective ones mention something specific you learned.
Use this structure:
- Open with appreciation for their time and access
- Name one concrete takeaway from the experience
- Close professionally without overreaching
Example:
Thank you for allowing me to shadow in your clinic. I learned a great deal from watching how you narrowed the differential through a focused history and then explained the plan in a way the patient could follow. I appreciated your time and willingness to teach.
That kind of message does more than say thanks. It shows that you observed with intent.
Be careful about recommendation letters
Not every shadowing physician should write for you. A letter is only worth pursuing if the physician knows you well enough to say something specific.
Ask only when:
- They've seen you more than once or over a sustained period
- They've interacted with you beyond brief hallway conversation
- They can comment on your professionalism, curiosity, and reliability
If you do ask, make it easy for them. Share your resume, your CV, a draft of your personal statement if relevant, and a short reminder of what you did during the experience. A practical guide on how to ask for a letter of recommendation can help you phrase that request in a way that's respectful and clear.
Log hours accurately
Shadowing should be recorded cleanly and accurately. Don't inflate your role. Observation is observation.
Track:
- Physician name and specialty
- Dates
- Setting such as outpatient clinic, hospital service, or OR
- Total hours
- A few reflection notes to help later with applications
Your log matters because memory fades fast. By the time you're filling out AMCAS or AACOMAS, separate experiences can blur together. Good notes preserve details that make your description credible.
Keep the language accurate. If you observed patient care, say that. Don't describe shadowing as direct patient care, clinical volunteering, or hands-on work if it wasn't.
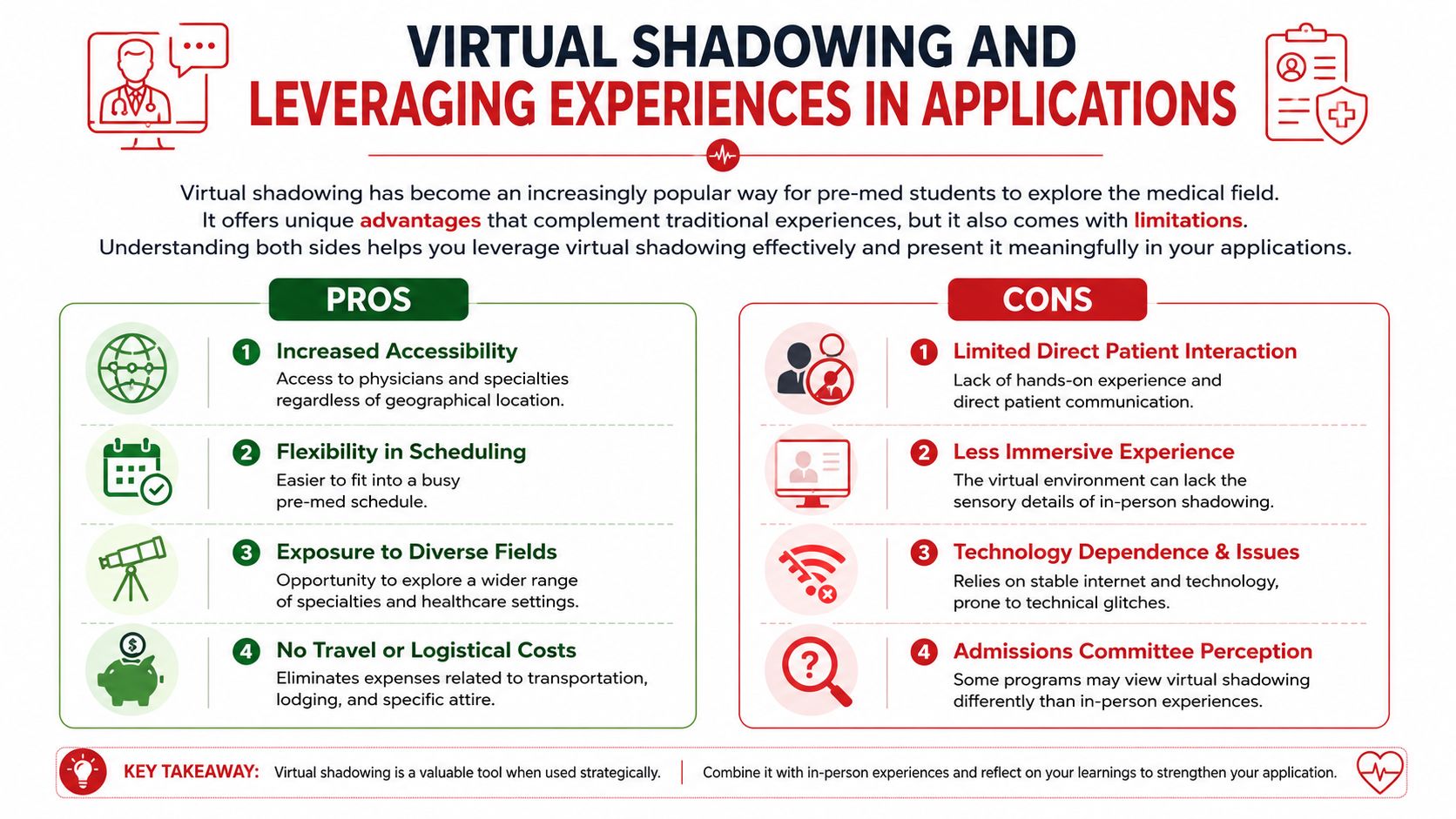
Virtual Shadowing and Leveraging Experiences in Applications
You finish a virtual shadowing session with solid notes on a chest pain workup, but then the doubt starts. Will this matter on an application? Did it teach enough compared with standing in clinic beside a physician?
Virtual shadowing has a real role. It expands access for students who live far from academic centers, have work or family obligations, or cannot arrange in-person exposure quickly. It also trains a different skill set. Because the screen strips away some of the room dynamics, many students pay closer attention to how the physician builds a differential, prioritizes data, and explains uncertainty. That matters for applications, and it matters for board prep.
The limitation is clear. Virtual experiences usually give less exposure to clinic flow, body language, team communication, and the pace of real patient care. In-person shadowing remains stronger for understanding how medicine feels in practice. Virtual sessions are often stronger for focused case teaching and for hearing a clinician explain why one diagnosis moves up the list while another drops off.
Compare format by what it teaches you
A useful way to judge shadowing is to ask what type of clinical reasoning each format strengthens.
In-person shadowing helps you study:
- How physicians gather clues before the formal presentation begins
- How patient communication changes the history you get
- How nurses, MAs, residents, and attendings shape decisions
- How time pressure affects diagnostic and treatment choices
Virtual shadowing helps you study:
- Case-based reasoning in a more distilled form
- Problem representation and differential diagnosis
- Specialties you may not have access to locally
- Patterns that connect directly to USMLE and COMLEX style thinking
That last point gets missed in many shadowing guides. If you listen carefully during a good virtual case discussion, you are often hearing board-style reasoning out loud. You hear illness scripts, rule-in and rule-out thinking, and the logic behind next-step testing. Students who write down those patterns often get more from shadowing than students who only count hours.
Turn experience into a usable narrative
Applications reward specificity. Your description should answer three practical questions:
- What did you observe?
- What did you learn about how physicians think and work?
- How did that experience change the way you study, choose activities, or understand patient care?
The third answer separates a generic entry from a strong one. “I confirmed my interest in medicine” says very little. A stronger reflection sounds like this: you noticed that the physician did not chase every possible diagnosis at once. They ranked the most likely and most dangerous options first, then asked targeted questions to narrow the field. That observation changed how you approach board questions, because you started organizing vignettes by problem representation instead of memorizing isolated facts.
That kind of detail also improves your written materials. If you are updating a CV or activity section, reviewing actionable healthcare resume examples can help you describe clinical exposure with accurate language that stays within the limits of an observer role.
Your descriptions should also fit the bigger admissions picture. Reviewing what medical schools look for in applicants helps you frame shadowing as evidence of maturity, reflection, and informed commitment, rather than as a disconnected list of hours.
Use virtual shadowing honestly
Admissions committees generally understand why virtual shadowing exists. The concern is not the format itself. The concern is overstatement.
State the experience clearly. If you observed telehealth visits, case conferences, or structured physician-led discussions, say that. Then explain what you learned from the physician's reasoning, communication, or approach to ambiguity. That is a credible and useful way to present the experience.
For medical students, the same rule applies later. Shadowing alone will not carry an application, but it can sharpen specialty understanding and strengthen the examples you use in personal statements, secondaries, and interviews. Used well, it also builds a habit that helps on exams. We watch how clinicians frame a case, decide what matters, and justify the next step. That is the same mental work we need for strong clinical reasoning on test day.
If you want structured help turning shadowing into better exam performance and stronger application narratives, Ace Med Boards offers support for board prep, admissions planning, and clinical learning strategy so you can connect what you observe in clinic to how you study and present yourself.